

IN RESPONSE to healthcare challenges presented by antibiotiresistant infections, increasingly more complex patients, and patient transfers from hospitals into long-term care facilities, the Centers for Medicare and Medicaid (CMS) is requiring that all federally supported skilled nursing facilities (SNFs) have a trained infection preventionist (IP) on staff by November 2019. Surveyors will require written infection prevention and control policies based on current evidence-based practice guidelines. This mandate provides an opportunity to create infection prevention strategies throughout the continuum of care.
In 2017, the infection prevention department at CarolinaEast Medical Center (a 350-bed, not-for-profit, full-service community hospital) began a collaborative journey that stopped an outbreak of deadly super-bugs in two SNFs, reduced surgical site infections (SSIs) in a third, and ultimately improved outcomes in a community of healthcare facilities.
Call to action
Approximately 12% of the overall discharges from CarolinaEast Medical Center go to SNFs. The medical center’s laboratory performs all of the cultures for the community SNFs, and the three hospital IPs (all RNs) monitor culture results as part of routine surveillance. In 2017, a pan-resistant Acinetobacter baumannii infection emerged at one of the SNFs and a multidrug-resistant A. baumannii, sensitive only to meropenem, emerged at another. Carbapenem-resistant Enterobacteriaceae was identified in both facilities. A third SNF experienced an SSI outbreak in orthopedic patients discharged for rehabilitation. On readmission interviews, patients reported and demonstrated improper bathing techniques or lack of skin cleansing at the SNF.
The combination of the SSI outbreak and the new multidrug-resistant organisms (MDROs) was a call to action for the hospital IPs. Even though the patients weren’t in the hospital, they might be admitted or readmitted and potentially transmit these organisms.
The hospital IPs contacted the Statewide Program for Infection Control and Epidemiology (SPICE), the North Carolina Department of Health and Human Services, and area health education consultants to brainstorm and assist in developing a collaborative process that would include local post-acute healthcare facilities. SPICE infection control assessment and response (ICAR) results were presented, and a targeted education plan was developed based on those results. (See About SPICE.) The education program would be provided by the hospital IPs free of charge to all local SNFs, and the SNF IPs would be recruited to partner with hospital IPs for a successful education program and strategy implementation.
Existing relationships between hospital acute care discharge planners and SNF staff provided an avenue to establish initial contact. At their scheduled monthly meeting, an invitation was extended to all those attending to participate in a collaborative project to examine best practices, reduce infections, and improve the continuum of care. ICAR data were shared, and an improvement proposal presented. One SNF was immediately motivated to participate and was instrumental in developing the process change. Four months later, a second facility came on board followed by a third after another 4 months.
In North Carolina, the Statewide Program for Infection Control and Epidemiology (SPICE) conducts on-site infection control assessment and response (ICAR) evaluations across the state in a variety of healthcare settings, including long-term care. ICAR, which is funded by the Centers for Disease Control and Prevention and North Carolina Division of Public Health, Communicable Disease Branch, is also available online for use when an on-site evaluation can’t be conducted.
The goal of ICAR evaluations is to identify opportunities for improving infection prevention practices across the continuum of healthcare. When evaluations are completed, facilities are provided with:
• a written report of the findings
• recommendations for improvement.
Facilities in North Carolina can access many resources related to infection control and long-term care, including free training modules, at spice.unc.edu/ltc.
Source: Statewide Program for Infection Control and Epidemiology. spice.unc.edu/about
Action plan
Surveillance data showed that during the 12 months before plan implementation, 13 patients were affected by the newly emerging organisms from two SNFs. Infections among these patients resulted in hospital admission for a variety of problems, including sepsis, surgery, and amputations. During the same period, an increase in patients with SSIs admitted from SNFs occurred, accounting for 57% of total SSIs.
A team of hospital and SNF IPs, along with members of SPICE and the North Carolina  Department of Public Health, identified strategies based on initial feedback from SNF staff, ICAR data, and surveillance data. SNF staff feedback was gathered through informal interviews, ICAR data were collected via the SPICE project, and surveillance data came from the hospital laboratory. The team then intervened with a multipronged approach targeting key areas through education and practice changes. (See Education plan of action.)
Department of Public Health, identified strategies based on initial feedback from SNF staff, ICAR data, and surveillance data. SNF staff feedback was gathered through informal interviews, ICAR data were collected via the SPICE project, and surveillance data came from the hospital laboratory. The team then intervened with a multipronged approach targeting key areas through education and practice changes. (See Education plan of action.)
Education format
The SNF schedule allowed for 15-minute concentrated, interactive education sessions. These sessions, which incorporated return demonstration, relatable practice stories, and visual tools that can be shared with others, helped build and establish relationships.
Each education session was designed to target a practice that had been identified as problematic in the ICAR data. Education was provided monthly for 6 months and then re-evaluated, and handouts were posted for reference. One IP at each SNF was the key contact for coordinating and evaluating interventions.
Practice changes
Top priorities for practice changes included bathing, wound care, environmental disinfection, communication, and decreasing organism transmission.
Bathing. Bath basins were being used and reused indefinitely; staff reported that they sometimes had residue on them. Practices changes included defining disposal days for basins along with more consistent cleaning techniques. One SNF changed to weekly basin changes; the others changed to single-basin use.
An abundance of evidence exists about chlorhexidine gluconate (CHG) bathing for healthcare-acquired infection (HAI) prevention and reduction in acute care settings, but less information is available about its use in SNFs. Based on acute care experience, the team agreed to implement 4% CHG daily bathing for high-risk patients (surgical rehabilitation patients and those known to be colonized or infected with an MDRO). Staff were taught about the evidence behind CHG and HAI prevention and provided with instructions for using CHG.
Wound care. Wound care practices were evaluated, and best practice opportunities were identified. Environmental cultures were collected from multiple surfaces and grew pathogens. Results were reviewed with staff, which led to conversations about the chain of infection and transmission. This discussion resulted in changes in wound care aseptic technique, including: • a clean area for each wound dressing change
• techniques to avoid tape contamination
• single-patient instruments for wound care.
Environmental disinfection. A. baumannii had been discussed during the MDRO education classes, including where it’s commonly found, the type of organism it is, and environmental factors that affect it. In one SNF, environmental services (EVS) was an isolated department with independent management that was responsible for all cleaning and disinfection. The SNF IP and hospital IP sought out the EVS staff to open lines of communication. Education about the importance of changing water and mop heads after cleaning an isolation room floor was reinforced.
 Communication. A communication breakdown between hospital and SNF staff was identified. Laboratory results were available in paper and electronic records sent to the SNF with the patients, but bed assignments had already been completed before the SNF staff had access to electronic health records (EHRs); in some cases, staff didn’t review the paper records in a timely manner. The team decided to use the EHR to improve communication. A notification is included in the EHRs of patients with an MDRO to alert the discharge planners, and the hospital and SNF IPs discuss risk factors and required measures before patients are discharged.
Communication. A communication breakdown between hospital and SNF staff was identified. Laboratory results were available in paper and electronic records sent to the SNF with the patients, but bed assignments had already been completed before the SNF staff had access to electronic health records (EHRs); in some cases, staff didn’t review the paper records in a timely manner. The team decided to use the EHR to improve communication. A notification is included in the EHRs of patients with an MDRO to alert the discharge planners, and the hospital and SNF IPs discuss risk factors and required measures before patients are discharged.
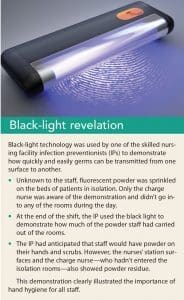
Decreasing organism transmission. To address the issue of organism transmission, the hospital IP introduced the SNFs to black-light technology to evaluate hand hygiene. In one of the most interactive and enlightening education sessions, fluorescent powder and black lights were used to demonstrate how easily organisms are transmitted out of patient rooms and into the rest of the facility. (See Black-light revelation.)
Outcomes and impact
In Phase 1 of the plan (9 months before implementing any interventions), 10 patients were known to be infected with newly emerging organisms. In Phase 2 (6 months during initial plan implementation), six patients were infected. No infections were reported during Phase 3 (8 months after complete implementation). The program resulted in a 90% reduction in MDRO infections and halted an outbreak in two SNFs. The facilities have maintained a zero-transmission rate for 6 months. The hospital has seen a 100% reduction in the number of SSI readmissions from the SNFs in the 8 months since full implementation of the project. (See Project outcomes.)
At the end of 12 months, everyone agreed that the program was helpful and should be continued for at least 12 more months. This model has implications for other acute and post-acute facilities. Reaching outside of an organization’s walls and working with community partners on shared issues using a multifaceted intervention plan are key elements for success.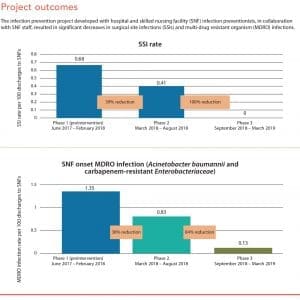
Shared vision
Project success requires collaboration. Hospital and SNF IPs worked in partnership to identify opportunities for process improvement. Their open, honest, no-judgment discussions created an atmosphere of staff empowerment that resulted in improved patient safety. The IPs continue to work together to address their common responsibility for infection prevention. Their shared vision has formed a foundation of trust and communication that benefits all patients.
Cathy Fischer is the manager, infection prevention at CarolinaEast Medical Center in New Bern, North Carolina. Jaime Drake is the registered nurse clinic competency coordinator at PruittHealth–Neuse in New Bern, North Carolina.
Selected references
Centers for Disease Control and Prevention. National Healthcare Safety Network (NHSN): Surveillance for surgical site infection (SSI) events. June 19, 2010. cdc.gov/nhsn/acute-care-hospital/ssi/index.html
Centers for Disease Control and Prevention. Management of Multidrug-Resistant Organisms in Healthcare Settings, 2006. Updated February 15, 2017. cdc.gov/infectioncontrol/pdf/guidelines/mdro-guidelines.pdf
Dumyati G, Stone ND, Nace DA, Cmich CJ, Jump RL. Challenges and strategies for prevention of multidrug-resistant organism transmission in nursing homes. Curr Infect Dis Rep. 2017;19(4):18.
Roghmann MC, Johnson JK, Sorkin JD, et al. Transmission of methicillin-resistant Staphylococcus aureus (MRSA) to healthcare worker gowns and gloves during care of nursing home residents. Infect Control Hosp Epidemiol. 2015;36(9):1050-7.
Scarborough P. Infection Prevention and Control: Overview of the New CMS Rules & Survey Process. Presented at: Health Care Association of New Jersey 69th Annual Convention; October 23-26, 2017; Atlantic City, NJ. hcanj.org/files/2013/10/Infection-Prevention-and-Control-Overview-of-New-CMS-Rules-and-Survey-Process-by-Pamela-Scarborough.pdf
Tian W. An all-payer view of hospital discharge to postacute care, 2013. Healthcare Cost and Utilization Project (HCUP) statistical brief #205. Agency for Healthcare Research and Quality. May 2016. hcup-us.ahrq.gov/reports/statbriefs/sb205-Hospital-Discharge-Postacute-Care.pdf.
Wang EW, Layon AJ. Chlorhexidine gluconate use to prevent hospital acquired infections—A useful tool, not a panacea. Ann Transl Med. 2017;5(1):14.
Wang J, Foxman B, Mody L, Snitkin ES. Network of microbial and antibiotic interactions drive colonization and infection with multidrug-resistant organisms. Proc Natl Acad Sci U S A. 2017;114(39): 10467-72.















