
A case report to guide nurse practitioners.
By Myriam Jean Cadet, PhD, APRN, MSN, FNP-C
Takeaways
- Early diagnosis of cystitis is important to manage and prevent renal complications.
- Antibiotic drug therapy can help provide a cure for cystitis.
- Nurses play a critical role in managing care of cystitis patients.
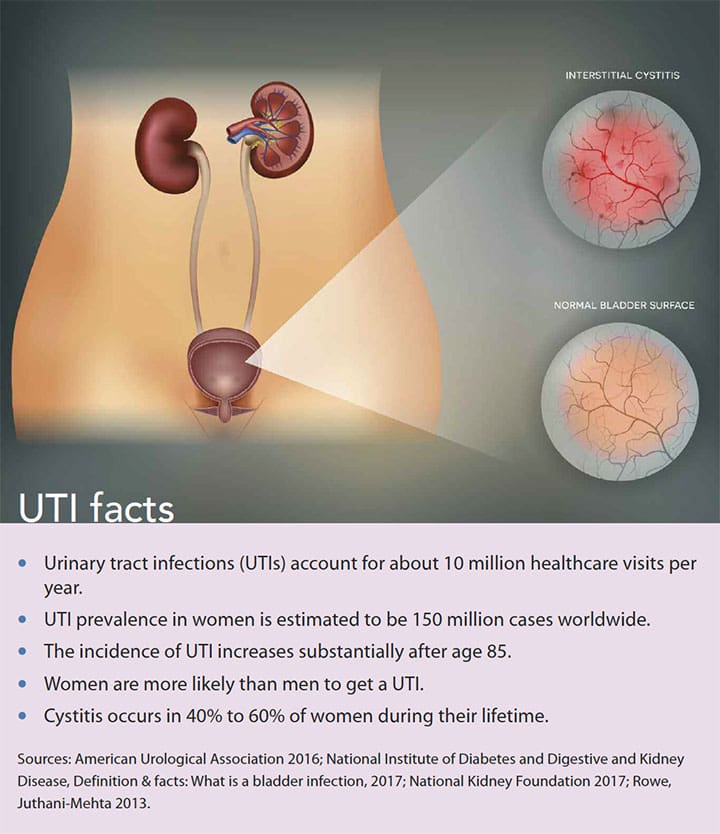
Cystitis (inflammation of the bladder) is a lower urinary tract infection (UTI) commonly caused by a uropathogenic agent such as Escherichia coli (E. coli). (See UTI facts.) Signs and symptoms include urinary urgency and frequency, as well as burning on urination. Untreated cystitis can lead to renal in-fections such as pyelonephritis, which is an upper UTI that affects the kidneys. As a nurse practitioner (NP), you’ll encounter this significant health problem in primary care settings. This article uses a case description to analyze NPs’ role in the diagnosis, treatment, and prevention of uncomplicated cystitis.
Discussion
Cystitis causes inflammation to the bladder and can be subclassified as complicated or uncomplicated. Patients with uncomplicated cystitis experience urinary incontinence, urgency, and burning on urination, which may persist for days or weeks. Complicated cystitis manifests with the same symptoms as uncomplicated cystitis, but additional characteristics include urinary obstruction, male gender, diabetes, history of drug resistance, recurrent cystitis, or pregnancy. Complicated cystitis may need more extensive evaluation and longer antibiotic treatment.
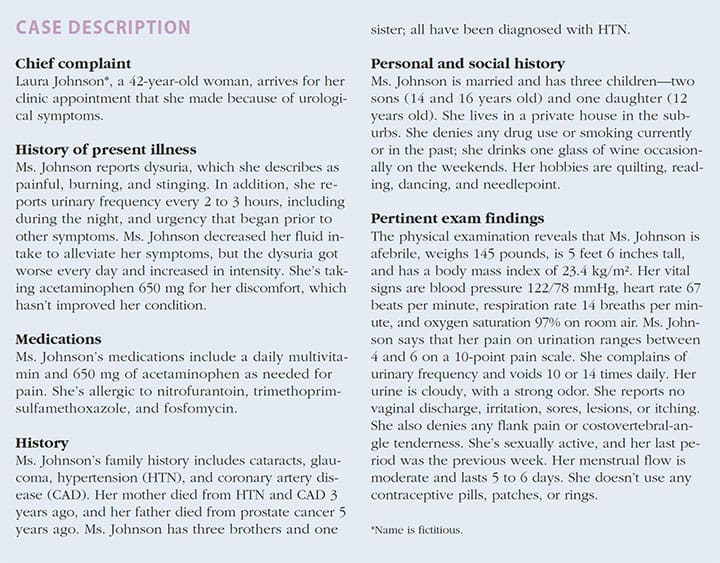
Adequately assessing cystitis can be challenging because symptoms overlap with other urologic conditions, such as pyelonephritis. As an NP, you should be prepared to initiate effective medical treatment to provide safe, quality care for patients with cystitis. We’ll use Ms. Johnson’s case of uncomplicated cystitis to guide your diagnosis and treatments.
Pathogenesis and etiology
Cystitis usually occurs when fecal flora colonize in the urethra and then ascend through the urinary tract into the bladder. E. coliaccounts for about 80% of all outpatient UTIs. Other uropathogens that cause cystitis are Staphylococcus, Proteus, Candida, Klebsiella, and Enterococcus. Women are predisposed to cystitis because their urethras are short and close to the anus, which facilitates the entry of bacteria into the urinary tract.
Behavioral and biologic factors may predispose patients to cystitis. Behavioral factors include urinary catheterization or sexual intercourse; biologic factors include structural abnormalities and metabolic or hormonal conditions. Other biologic factors include spinal cord injury, renal calculi, transplant, cysts, urinary incontinence, prostate enlargement, kidney stones, urinary obstruction, pyelonephritis, diabetes, AIDS, and pregnancy.
Other potential predisposing factors for cystitis include age, reduced mobility, changes in acidity in the vagina, and being premenopausal.
Ms. Johnson’s risk factors for uncomplicated cystitis include being female and sexually active.
Differential diagnoses
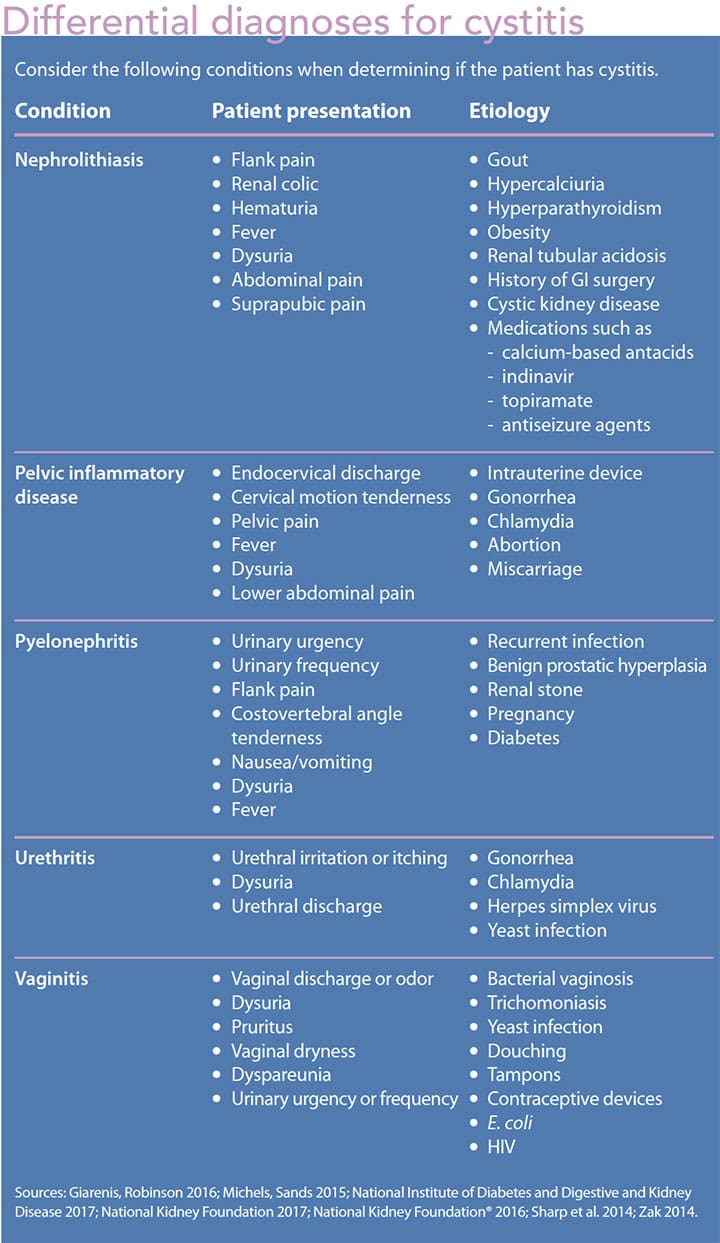
Differential diagnoses include urethritis, vaginitis, pelvic inflammatory disease, nephrolithiasis, and pyelonephritis. All have been associated with dysuria, but dysuria usually is caused by urethritis, vaginitis, cystitis, or pyelonephritis. Dysuria, vaginal discharge, sexually transmitted infection, irritation, and itching may be related to urethritis or vaginitis (candidiasis or trichomonas vaginitis). A patient who presents with dysuria, flank pain, fever, and chills, and who looks ill may have pyelonephritis. (See Differential diagnoses for cystitis.)
Diagnosis
Ms. Johnson’s symptoms of urinary urgency and frequency in addition to dysuria are consistent with a diagnosis of uncomplicated cystitis. To confirm this diagnosis, a urine dipstick, microscopic urine analysis, or urine culture may be ordered. Im-aging studies aren’t recommended for uncomplicated cystitis.
Urine dipstick
A urine dipstick checks for urine pH, glucose, protein, bilirubin, blood, and white blood cells (WBCs). It’s the simplest tool to screen for cystitis, but its low specificity and sensitivity may generate false results. Positive leukocyte esterase and nitrite tests from a urine dipstick may indicate cystitis, but they also may indicate bacterial growth and pyuria. However, negative test results, when combined with positive clinical presentations, don’t rule out cystitis.
Ms. Johnson’s urine dipstick results are positive for leukocyte esterase and nitrite, so cystitis treatment should be considered.
Microscopic urinary analysis
A microscopic exam measures red blood cells (RBCs) and WBCs in the urine and detects casts, bacteria, hematuria, and crystals.
Ms. Johnson’s urinary sediment results are positive for WBCs, RBCs, and bacteria, which may be associated with cystitis.
Urine culture
A urine culture is a definitive diagnostic test to guide drug treatment and provide a cure for UTIs. It helps determine the source of infection, so that proper antibiotic treatment can be ordered, thereby avoiding unnecessary therapy. A urine culture of > 10 5 CFU/mL is diagnostic for UTIs.
A culture was not needed in Ms. Johnson’s case because her cystitis was considered uncomplicated; a urine cultures is used to diagnose complicated cystitis.
Managing uncomplicated cystitis
Antibiotic treatment goals for cystitis include relieving symptoms, preventing bacterial resistance and kidney complications, and curing the infection. Local resistance rates, bacterial pathogens (if known), patient allergies and comorbidities, drug costs and adverse effect profiles, and history of medication adherence should guide your choice of antibiotic treatment.
A 3-day course of antibiotic therapy, as recommended by the Infectious Diseases Society of America 2011 guidelines, usually is sufficient to eradicate uncomplicated cystitis. (See Treatment options.)
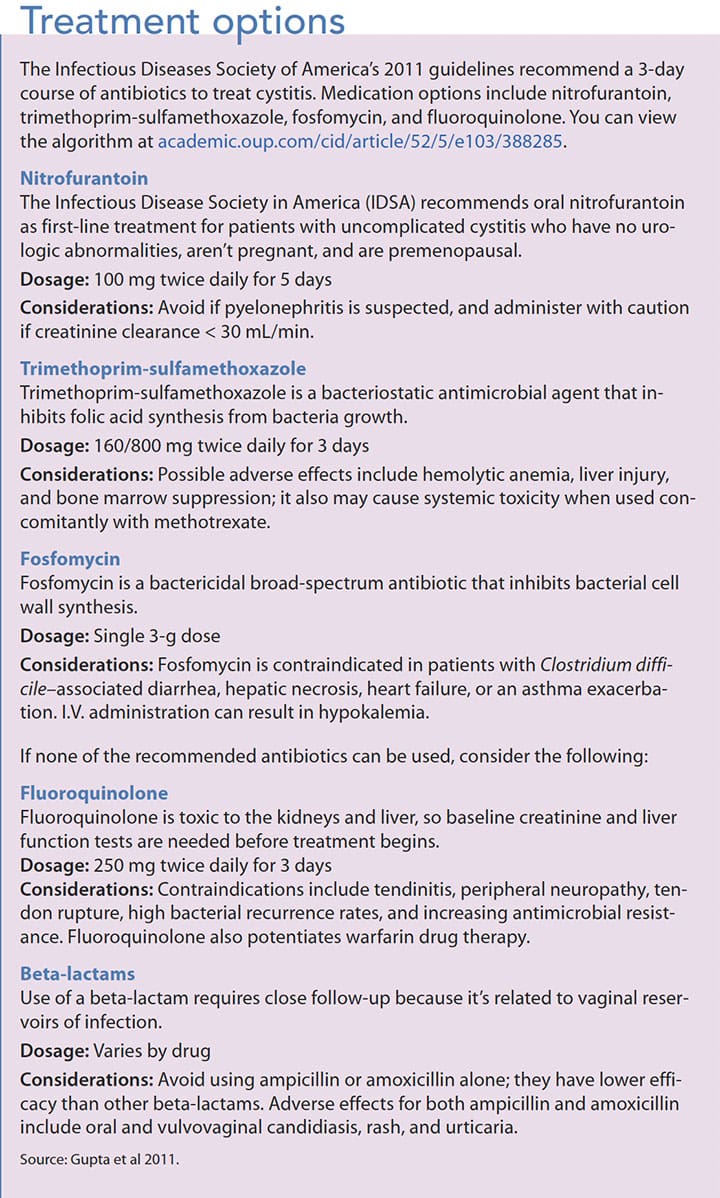
Based on Ms. Johnson’s diagnosis and allergies to nitrofurantoin, trimethoprim-sulfamethoxazole, and fosfomycin, you prescribe a 3-day course of fluoroquinolone 250 mg twice daily.
Education and prevention
Prevention begins with education. Explain to patients that treatment adherence will help prevent reinfection and relapse of cystitis. Instruct them to take the full course of antibiotics to cure the infection and prevent antimicrobial resistance. In addition, review possible medication adverse effects and when the patient should seek help. Patients with complicated cystitis should have a repeat urine culture to confirm the infection is cured.
Suggest other steps patients can take at home to prevent cystitis, such as drinking adequate amounts of water to help clear bacteria from the body. This is especially important for someone who has difficulty emptying his or her bladder because of conditions such as bladder spasms. Other preventive measures include cleaning the perineal area as needed, wiping from front to back after urinating, changing underwear every day, and cleaning with soap and water after each bowel movement.
Some patients benefit from cranberry products, which acidify the urine and inhibit bacterial growth in the bladder. In one study, cranberry juice consumption for 8 weeks (4 ounces daily) significantly reduced UTI symptoms among 24 female participants. However, another study acknowledged that cranberry products have limited evidence in cystitis prevention.
For patients with recurrent UTIs, prescribe a bactericidal prophylaxis antibiotic therapy. Methenamine 1 g by mouth four times daily can be used as a preventive therapy. Refer patients with recurrent UTIs to urology or urogynecology for further evaluation.
When Ms. Johnson returned for her next office visit for a routine checkup, she reported that she had had no further episodes of infection.
Role of NP
Through careful assessment, diagnosis, and education, NPs can ensure that patients with cystitis are successfully treated. Taking the additional step of explaining self-care actions also can promote a positive outcome and lay the groundwork for preventing recurrence of infection and antibiotic resistance.
Myriam Jean Cadet is a family nurse practitioner and an adjunct professor at Lehman College in Bronx, New York.
Selected references
American Urological Association. Medical student curriculum: Adult UTI. 2016.
Axelsson M. Report on personality and adherence to antibiotic therapy: A population-based study. BMC Psychol. 2013;1(1):24.
Bates BN. Interpretation of urinalysis and urine culture for UTI treatment. US Pharm. 2013;38(11):65-8.
Bass-Ware A, Weed D, Johnson T, Spurlock A. Evaluation of the effect of cranberry juice on symptoms associated with a urinary tract infection. Urol Nurs. 2014;34(3):121-7.
Cudmore J, Seftel M, Sisler J, Zarychanski R. Methotrexate and trimethoprim-sulfamethoxazole: Toxicity from this combination continues to occur. Can Fam Physician. 2014;60(1):53-6.
Curtiss N, Meththananda I, Duckett J. Urinary tract infection in obstetrics and gynaecology. Obstet Gynaecol Reprod Med. 2017;27(9):261-5.
European Association of Urology. EAU guidelines on urological infections. 2016.
Falagas ME, Vouloumanou EK, Samonis G, Vardakas KZ. Fosfomycin. Clin Microbiol Rev. 2016;29(2):321-47.
Flores-Mireles AL, Walker JN, Caparon M, Hultgren SJ. Urinary tract infections: Epidemiology, mechanisms of infection and treatment options. Nat Rev Microbiol. 2015;13(5):269-84.
Frieder J, Mouabbi JA, Zein R, Hadid T. Autoimmune hemolytic anemia associated with trimethoprim-sulfamethoxazole use. Am J Health Syst Pharm.2017;74(12):894-7.
Giarenis I, Robinson D. Lower urinary tract infections. In: Luesley DM, Kilby MD, eds. Obstetrics & Gynaecology: An Evidence-based Text for the MRCOG. 3rd ed. Boca Raton, FL: CRC Press; 2016; 773-9.
Grigoryan L, Trautner BW, Gupta K. Diagnosis and management of urinary tract infections in the outpatient setting: A review.JAMA. 2014;312(16):1677-84.
Gupta K, Hooton TM, Naber KG, et al; Infectious Diseases Society of America; European Society for Microbiology and Infectious Diseases. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: A 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin Infect Dis. 2011;52(5):e103-20.
Heidelbaugh JJ, Holmstrom H. The perils of prescribing fluoroquinolones. J Fam Pract. 2013;62(4)191-7.
Lo TS, Hammer KD, Zegarra M, Cho WC. Methenamine: A forgotten drug for preventing recurrent urinary tract infection in a multidrug resistance era. Expert Rev Anti Infect Ther. 2014;12(5):549-54.
Michels TC, Sands JE. Dysuria: Evaluation and differential diagnosis in adults. Am Fam Physician.2015;92(9):778-86.
Mody L, Juthani-Mehta M. (2014). Urinary tract infections in older women: A clinical review. JAMA.2014;311(8):844-54.
National Institute of Diabetes and Digestive and Kidney Diseases. Definition & facts: What is a bladder infection?2017.
National Institute of Diabetes and Digestive and Kidney Diseases. Treatment: How do health care professional treat a bladder infection? 2017.
National Kidney Foundation®. Urinalysis and Kidney Disease: What You Need to Know. 2014.
Nicolle LE. Urinary tract infection. Crit Care Clin.2013;29(3):699-715.Oliphant CM, Eroschenko K. Antibiotic resistance, part 1: Gram-positive pathogens. J Nurse Pract. 2015;11(1):70-8.
Oliphant CM, Eroschenko K. Antibiotic resistance, part 2: Gram-negative pathogens. J Nurse Pract. 2015;11(1):79-86.
Rowe TA, Juthani-Mehta M. Urinary tract infection in older adults. Aging Health. 2013;9(5):519-28.
Sharp VJ, Lee DK, Askeland EJ. Urinalysis: Case presentations for the primary care physician. Am Fam Physician. 2014;90(8):542-7.
Shin CN. The effects of cranberries on preventing urinary tract infections. Clin Nurs Res. 2014;23(1):54-79.
Slim R, Asmar N, Yaghi C, Honein K, Sayegh R, Chelala D. Trimethoprim-sulfamethoxazole-induced hepatotoxicity in a renal transplant patient. Indian J Nephrol. 2017;27(6):482-3.
Tsai JD, Lin CC, Yang SS. (2016). Diagnosis of pediatric urinary tract infections. Urol Sci. 2016;27(3):131-4.
Velez R, Richmond E, Dudley-Brown S. Antibiogram, clinical practice guidelines, and treatment of urinary tract infection. J Nurse Pract. 2017;13(9):617-22.
Zak D. Managing uncomplicated recurrent urinary tract infections in reproductive aged women: A primary care approach. J Am Assoc Nurse Pract. 2014;26(12):658-63.
ant7-Cystitis-618
















