

Adults with psychiatric conditions who are admitted as inpatients need to be assessed carefully to ensure they receive the best possible care. Although staff nurses don’t make the diagnosis, your assessment can help the psychiatrist and other treatment team members understand the patient’s struggle. This is particularly important as many inpatients are hospitalized involuntarily and timely intervention is essential. (See Involuntary psychiatric admissions.) This article provides an overview of selected psychiatric conditions and their signs and symptoms.
Schizophrenia and schizoaffective disorder
Clinicians consider five domains when assessing patients for schizophrenia or schizoaffective disorder— delusions, hallucinations, disorganized thinking and speech, grossly disorganized or abnormal motor behavior (including catatonia), and negative symptoms.
• Delusions are fixed beliefs not amenable to change even in light of conflicting evidence (excluding religious beliefs commonly held in the community).
Examples include:
• delusions of persecution (“someone is out to get me”)
• nihilistic delusions (“something bad is going to happen”)
• somatic delusions (“something is terribly wrong with me”)
• control delusions (“someone is making me do something”)
• thought-withdrawal delusions (“aliens are stealing my thoughts”)
• thought-insertion delusions (“aliens are putting thoughts into my head”)
• thought-broadcasting delusions (“everyone can hear my thoughts”)
• referential delusions (“people are talking about me”)
• delusions of grandeur (for instance, a patient thinks she’s royalty and should be treated as such)
• erotomania (a false belief that others are in love with the patient).
• Hallucinations are perception-like experiences that occur without an external stimulus. In schizophrenics, auditory hallucinations (AHs) are more common than visual or other hallucinations. Visual hallucinations (VHs) may be illusions (misinterpretation of visual stimuli; for instance, a shadow becomes a menacing black dog). VHs can occur with other medical conditions, such as alcohol withdrawal, or may manifest as an aura with a seizure or brain injury. AHs and VHs rarely occur at the same time.
• Disorganized thinking and speech may include:
• circumstantiality (verbalization of concrete details that’s slow in getting to the point)
• concrete thinking (making literal rather than figurative interpretations; for instance, the patient answers “I took the bus” when asked how he or she ended up in the hospital)
• clang associations (rhyming words and not completing sentences)
• loose associations (sentences or phrases not logically connected to those coming before or after)
• tangentiality (going from topic to topic without making a point)
• neologisms (making up words that have meaning only to the patient)
• “word salad” (a stream of unconnected words).
• Grossly disorganized and abnormal motor behavior may manifest as:
• unpredictable behavior that interferes with task completion or causes agitation
• failure to follow instructions to move
• holding a fixed bizarre position
• lack of verbal or physical response
• purposeless or repetitive movements
• staring at staff
• catatonic stupor not caused by a physical problem.
• Negative symptoms refer to lack of something, including:
• lack of emotional expressions
• avolition (lack of motivation for goal-oriented tasks)
• alogia (decreased speech)
• anhedonia (lack of pleasure from activities previously enjoyed)
• asociality (lack of interest in others).
A schizophrenic patient with negative symptoms seems to lack personality.
Signs and symptoms of schizophrenia and schizoaffective disorder
Signs and symptoms of schizophrenia include delusions, hallucinations, disorganized speech, and grossly disorganized or catatonic behavior.
Signs and symptoms of schizoaffective disorder include:
• a major mood episode of either major depression or mania for at least 1 month
• at least 2 weeks of delusions or hallucinations that don’t occur at the same time as a major mood episode.
Assessment tips
If your patient seems to be hearing voices, observe him or her to determine the following:
• Is the patient talking to a wall or an empty space?
• Is he or she mumbling or yelling? If so, can you make out words or themes?
• Are the patient’s eyes darting, staring, or frightened?
• Does the patient seem to be lost in thought?
• Is the patient thought blocking (stopping talking abruptly)?
• What is the patient’s affect (nonverbal expression of feelings, including posture, facial expression, and tone of voice)?
Try to determine if the patient seems internally preoccupied or is behaving in a way that’s consistent with AHs. Once you’ve formed general impressions, ask the patient questions such as the following:
• Are the voices frightening?
• What are they saying?
• Are they telling you to do something?
• Are they loud?
• Do you believe the voices?
• How often do you hear them?
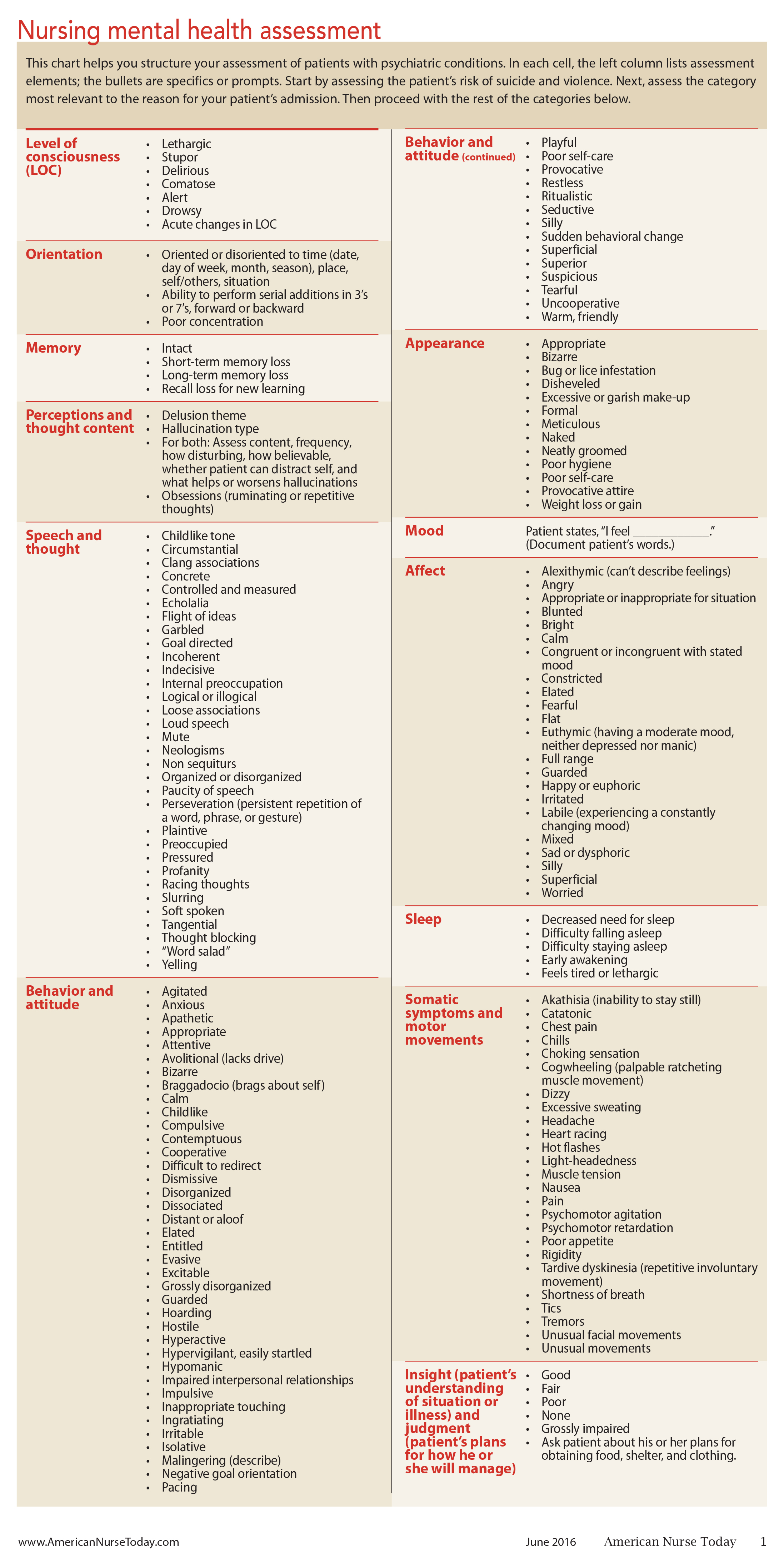
Keep in mind that paranoid patients may not admit to hearing voices until they’ve developed trust in you or until antipsychotic medications start to take effect. Try to identify a theme to what the voices are saying; for example, are they worried something bad will happen? Unfortunately, voices rarely go away completely even when the patient is well-managed on medications. (Download Nursing mental health assessment.)
Bipolar I disorder
Bipolar I disorder involves manic episodes that last at least 1 week or manic symptoms severe enough to require immediate hospital care. Mixed episodes (mania and depression at the same time) may occur as well. Some patients also experience episodes of hypomania (similar to mania but less intense). The episodes don’t stem from a medical condition or substance use.
Signs and symptoms
The following are examples of signs and symptoms of bipolar I disorder:
• persistent elevated mood, including high energy output, expansiveness, persistence, task and goal orientation, or marked irritability
• significant behavior changes, such as grandiose behavior, constantly moving without purpose, taking part in high-risk activities, such as sex with strangers, or incessant rapid speech.
In many cases, patients with bipolar disorder require hospitalization to protect themselves from their own behavior.
Assessment tips
When assessing the patient, ask yourself these questions:
• What is the patient’s mood? (Document this in the patient’s own words.)
• What is the patient’s affect? (How does the patient appear to be feeling?)
• What is the quality and content of the patient’s behavior and speech?
Documentation tips
Describe specific risks of the patient’s manic behavior, including sexual risks, antagonizing others, making intrusive phone calls, making life-defining decisions, or losing weight because the patient can’t sit long enough to eat a meal. Keep in mind that a patient with bipolar I disorder may be in the depressed phase of the condition, so be sure to assess for depression, suicide risk, and marked shifts in mood or affect. (See Assessing the patient’s violence and aggression risk.) When documenting the quality and content of the patient’s behavior and speech, be as specific as possible.
Major depressive disorder
Major depressive disorder causes severe symptoms that affect how the patient thinks and feels. It also may affect such activities as sleeping, eating, and working. The patient must have signs or symptoms for at least 2 weeks. In 2014, an estimated 15.7 million adults aged 18 or older in the United States had at least one major depressive episode in the past year, making it one of the most common mental health disorders.
Essential information to communicate during care transitions includes:
• pain management history
• pain assessment tools and scales used
• complementary and pharmacologic interventions tried and shown to be either effective or ineffective
• patient goals for pain outcomes.
Clinical decision-making tools, such as alerts in the electronic health record regarding inappropriate or high-alert medications, flag alerts for frail elders, and embedded standard communication and pain assessment tools, may promote effective communication and documentation.
Signs and symptoms
Patients with a major depressive disorder have a depressed mood or loss of pleasure or interest in activities that usually provide pleasure. Other signs and symptoms include:
• unintentional weight loss or gain (5% or more in 1 month)
• insomnia or hypersomnia
• psychomotor agitation
• fatigue
• feelings of worthlessness or excessive guilt
• decreased ability to concentrate
• suicidal thoughts or a suicide attempt.
Be aware that depression differs from dementia and delirium. Dementia is a gradual neurocognitive decline involving decreased logic and memory; for instance, patients try to answer questions but give the wrong answer. Delirium is marked by sudden onset of rapid fluctuations in behavior and level of consciousness; it stems from medication, substance use, or a medical condition. Delirium usually is a medical emergency.
Assessment tips
When assessing patients with a suspected major depressive disorder, start by evaluating their risk for suicidal ideation or behavior. (See Suicide risk assessment.) Ask the patient how he or she is feeling, and document the answer in the patient’s own words; for instance, “Patient states that mood is ________.”
Also ask the patient to rate his or her mood on a scale of 1 to 10, with 10 indicating the most severe feelings of depression. Note the patient’s affect (how he or she appears to be feeling) and determine if it matches the stated mood.
Next, assess the amount and pattern of the patient’s sleep, fluid and food intake, recent weight changes, activity and behavior level, and self-care (noting how much prompting or assistance the patient needs).
Keep in mind that depressed patients typically give brief answers or may say they don’t care or don’t know the answer. Also, patients with depression who have an unknown history of manic or hypomanic episodes may be tipped into a manic phase when they begin antidpressants without also taking mood-stabilizing medication.
Alcohol withdrawal syndrome
Alcohol withdrawal syndrome occurs when a person reduces or stops consuming alcohol, especially after a period of heavy or prolonged drinking. Severe withdrawal symptoms require medical attention and possibly hospitalization for detoxification.
Signs and symptoms
The following may occur with alcohol withdrawal syndrome:
• autonomic hyperactivity (diaphoresis, increased pulse)
• tremor (usually of the hands)
• insomnia
• nausea and vomiting
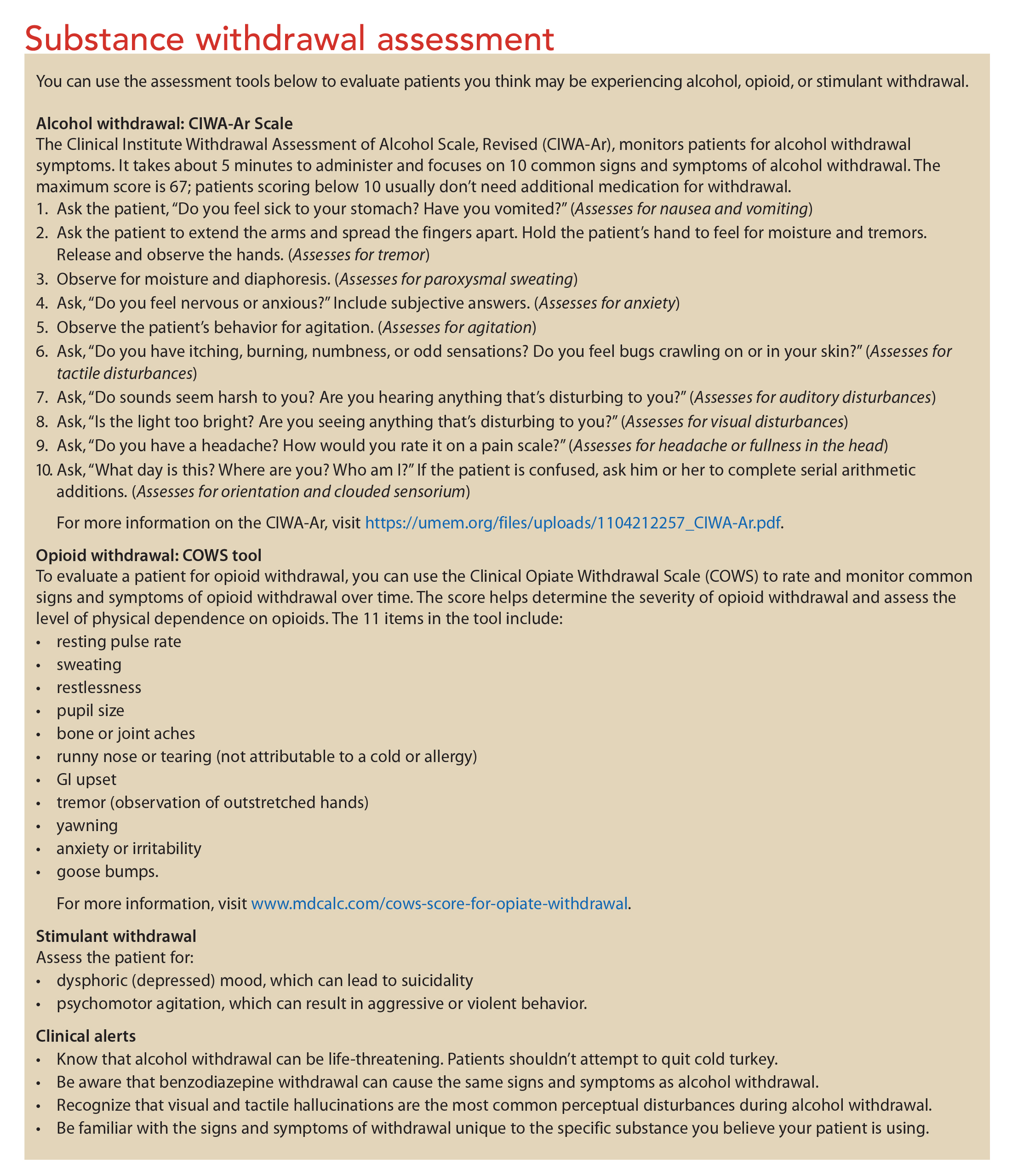
• hallucinations or illusions, which typically start as sensitivity (for instance, the patient complains that lights are too bright or sounds are too loud) and then develop into hallucinations (usually tactile or visual). Other signs and symptoms include anxiety, general tonic-clonic seizures, inability to sit still, and constant purposeless movement or fidgeting. (For more information on alcohol, opioid, and stimulant withdrawal, see Substance withdrawal assessment.)
Opioid withdrawal
Opioids include heroin, methadone, oxycodone, hydrocodone, and certain other substances. Heavy opioid use over several weeks changes brain chemistry. Opioid withdrawal occurs when the person stops using opioids.
Signs and symptoms
Patients with opioid withdrawal may have insomnia or a sad or depressed mood. Physiologic signs and symptoms may include:
• nausea and vomiting
• muscle ache
• lacrimation (tearing eyes)
• rhinorrhea (running nose)
• pupil dilation
• piloerection
• diaphoresis
• diarrhea
• yawning
• fever.
Stimulant withdrawal
Stimulants include amphetamine, methylphenidate (Ritalin), amphetamine with dextroamphetamine (Adderall), cocaine, and certain other substances. They cause changes in brain chemistry after short periods of use and have a short half-life. Withdrawal occurs after the person stops using stimulants.
Signs and symptoms
Patients with stimulant withdrawal may have a dysphoric mood along with:
• vivid and scary dreams
• insomnia or hypersomnia
• increased appetite
• psychomotor retardation
• inability to sit still
• constant purposeless movement or fidgeting.
Key points to remember
When assessing patients for mental illness or substance withdrawal, always assess the risk for suicidal and aggressive behavior, regardless of the patient’s specific diagnosis. Also, be aware that a patient may not admit to experiencing certain symptoms until he or she trusts you. Finally, be sure to fully document your observations in the health record so psychiatric physicians and nurse practitioners can more easily diagnose the patient’s specific problem using the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5).
Selected references
American Psychiatric Association. Diagnostic and Statitical Manual of Mental Disorders: DSM-5. 5th ed. Washington, DC: American Psychiatric Publishing; 2013.
Coombs T, Curtis J, Crookes P. What is the process of a comprehensive mental health nursing assessment? Results from a qualitative study. Int Nurs Rev. 2013;60(1):96-102.
Hutchinson K. Psychiatric-Mental Health Nursing: Nursing Review and Resource Manual. 5th ed. Silver Spring, MD: American Nurses Credentialing Center; 2015.
Jacobsen F. Type II workplace violence in an urban acute hospital: how do we know if we are creating a safer environment for patients and staff? J Safe Manag Disrup Assault Beh. 2012;20(2):4-8.
Jacobsen F, Adler J, Ortega JS. CIWA-Ar Training
. San Francisco, CA: CPMC Sutter Psychiatry; June 19. 2012.
National Institute of Mental Health. Major depression among adults.
Pederson DD. PsychNotes: Clinical Pocket Guide. 4th ed. Philadelphia, PA: F.A. Davis Company; 2013.
Townsend MC. Psychiatric Mental Health Care: Concepts of Care in Evidenced-Based Practice. 8th ed. Philadelphia, PA: F.A. Davis; 2015.
M. L. Feodora Jacobsen is chief nursing officer at Aurora Santa Rosa Hospital in Santa Rosa, California.
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
3 Comments.
I work at a acute psych facuilty and I love the information you have shared
please send mail
Very good article on assessment techniques related to the various mental health diagnosis to chemical dependency.