
A preventable and treatable lung disorder of adults, chronic obstructive pulmonary disease (COPD) is one of the most common causes of hospitalizations and readmissions. It affects 15 million Americans; nearly one in five hospital patients older than age 40 is diagnosed with the disorder.
In 2008, COPD surpassed stroke to become the third leading cause of death, after heart disease and all cancers combined. The disorder disproportionately affects women, the elderly, people without high-school diplomas, and those who are unemployed or living in households with annual incomes below $25,000.
In 2010, COPD healthcare expenditures and indirect costs (lost work and productivity) came to an estimated $36 billion. Experts project that by 2020, this figure will rise to about $49 billion.
In COPD hospital patients who develop respiratory failure and require mechanical ventilation, the mortality rate is about 30%. Among those who survive to discharge, the 1-year mortality ranges from 7% to 50% depending on severity of COPD exacerbations, comorbid conditions, and socioeconomic level.
Defining COPD
Marked by persistent airflow obstruction, COPD usually is progressive and associated with chronic respiratory symptoms. In the United States, tobacco smoking is the primary cause. Other risk factors include inhaled pollutants (such as occupational, indoor, and outdoor irritants) and genetic factors.
COPD is an umbrella term for two conditions—chronic bronchitis (a clinical diagnosis) and emphysema (a radiographic or pathologic diagnosis). In chronic bronchitis, airway inflammation and mucus plugging increase airway resistance and worsen airflow obstruction. In emphysema, destruction of the alveolar septa reduces gas exchange capacity and decreases elastic recoil after lung inflation, causing air trapping and hyperinflation.
Cycle of exacerbations and readmissions
Most COPD-related morbidity and mortality stem from exacerbations, marked by worsening respiratory symptoms, including difficulty breathing and excess phlegm production. Symptom burden from exacerbations may last days to 3 months or even longer, depending on disease severity, the patient’s functional status before the exacerbation, and comorbid conditions (for instance, heart failure).
COPD exacerbations lead to more year, with an in-hospital mortality of about 2.5%. About 20%, 30%, and 40% of patients hospitalized for exacerbations are readmitted at 1, 3, and 12 months, respectively. A large study of Medicare beneficiaries hospitalized for exacerbations found that 28% of readmissions within 30 days of discharge stemmed from worsening COPD. Other causes of readmission included respiratory failure, pneumonia, heart failure, comorbid asthma, sepsis, arrhythmias, and other conditions.
Factors associated with a higher risk of 30-day readmission include male sex, black race (vs. white), more comorbid conditions (including depression and heart failure), lower socioeconomic status (as assessed by Medicaid and Medicare co-enrollment), and worse health on discharge (measured by the need for skilled nursing or home care).
The Centers for Medicare & Medicaid Services (CMS) recently established the Hospital Readmissions Reduction Program to reduce readmission of patients hospitalized for COPD, acute myocardial infarction, pneumonia, and heart failure. In 2012, the program began imposing penalties for readmissions—an approach that left healthcare systems scrambling to find and implement evidence-based interventions to decrease avoidable readmissions.
Clinical presentation
COPD patients may have varying degrees of chronic bronchitis and emphysema, which together lead to chronic respiratory symptoms and difficulty breathing. According to the Global Initiative for Chronic Obstructive Lung Disease (GOLD), a ratio of forced expiratory volume in 1 second (FEV1) to forced vital capacity (FVC) of less than 0.70 indicates airflow obstruction—a criterion for COPD diagnosis.
Dyspnea (shortness of breath) is the hallmark of COPD—and a common impetus to seek medical attention. Perception of dyspnea varies from one person to the next and may not correlate with COPD severity. Dyspnea has a psychological component involving fear and anxiety related to the perception of breathlessness. Many persons with COPD initially limit themselves and their activities due to dyspnea and then abandon activity altogether, leading to more long-term disability.
Other signs and symptoms include cough and sputum production. Cough may be productive or nonproductive; chronic cough that produces sputum indicates chronic bronchitis.
Barriers to effective hospital-tohome transitions
Appropriate interventions can help overcome barriers to effective care transitions among COPD patients. Barriers may be patient-related or provider-related.
Patient-related barriers
In some patients, barriers to an effective transition include:
• COPD severity
• limited socioeconomic resources (such as income, home, or food insecurity and limited health literacy)
• comorbid conditions, which can greatly complicate management of exacerbations and necessitate an interprofessional care model in which nursing, social work, respiratory therapy, primary care and specialist clinicians, and others collaboratively develop care-transition strategies.
The case study below demonstrates the need to consider interventions directed at patient-related factors when developing a strategy of care for patients with COPD exacerbations.
Mr. B, a 72-year old African- American male, presents to the emergency department (ED) with severe dyspnea, increased sputum volume, and increased sputum purulence. He has a history of tobacco use. This is his fifth all-cause hospitalization in the past 12 months.
After he is admitted to the intensive care unit, Mr. B receives oral corticosteroids, antibiotics, nebulized bronchodilators, and noninvasive ventilation. He responds well to the treatment plan and is discharged home, with nebulizer and inhaled medications (an inhaled corticosteroid and bronchodilator) to be mailed to his house using next-day service.
About 10 days later, Mr. B comes to the ED again, complaining of shortness of breath and activity intolerance. He tells ED staff he never received the medications that were supposed to be mailed to his home. He says he seldom gets packages delivered at home because of widespread theft and vandalism in his neighborhood.
Provider-related barriers
Various studies have identified provider-related gaps in the quality of care and inadequate access to care after hospital discharge as key factors contributing to ineffective
care transitions. Such gaps can arise from breakdowns in communication, patient education, and accountability.
Communication breakdowns occur when clinicians fail to provide timely, effective, and complete information among themselves, the patient, and those who will care for the patient at home. Key risk factors for communication breakdowns include:
• differing expectations between senders and receivers during patient care transitions
• lack of teamwork
• insufficient time for successful transitions
• lack of standardized protocols for conducting successful transitions.
Patient education breakdowns occur when patients, caregivers, or both receive inadequate or conflicting recommendations about complicated medication regimens or unclear or absent follow-up instructions.
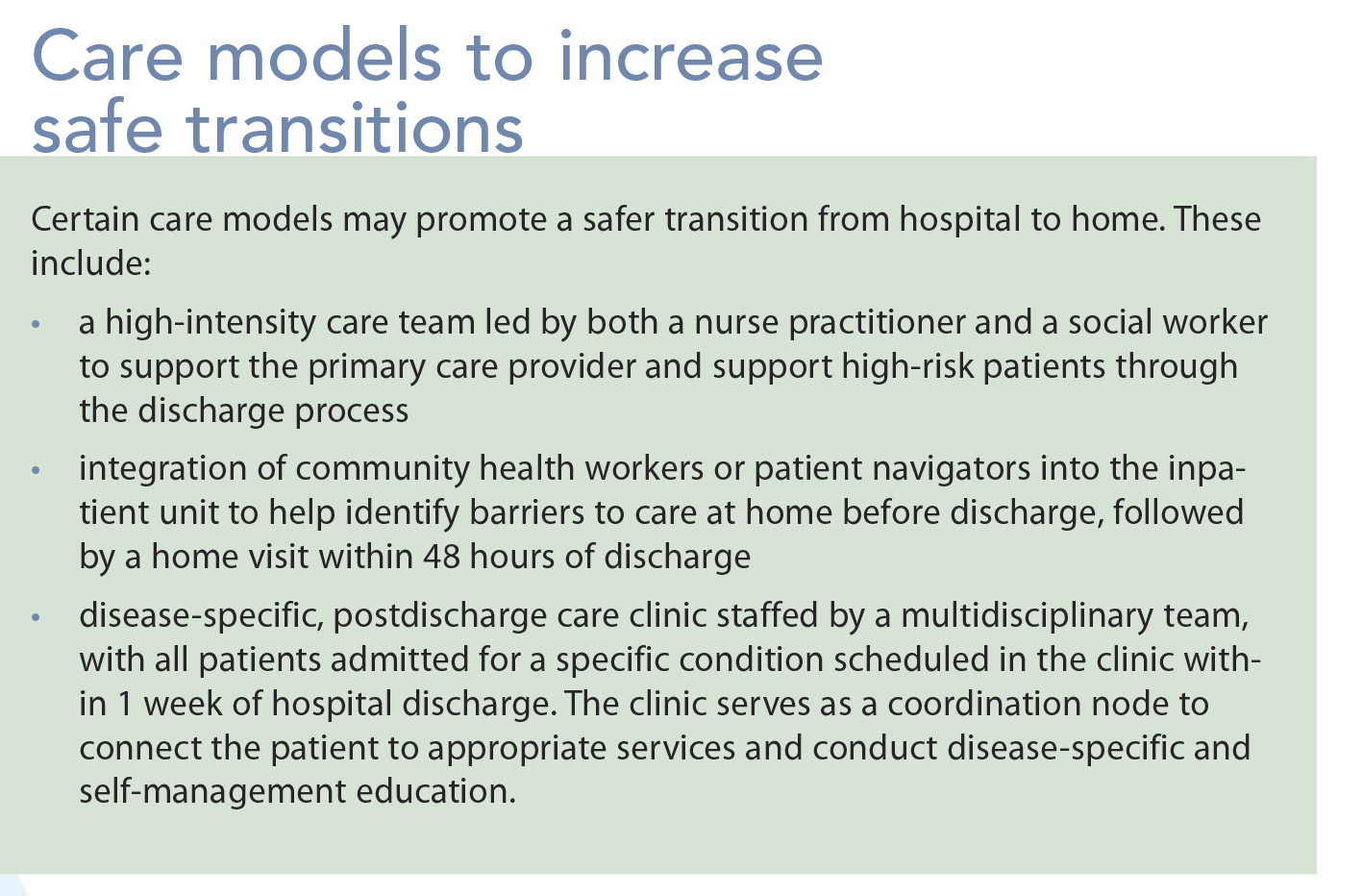
Accountability breakdowns occur when no clinical entity takes responsibility for coordinating the patient’s care across various settings (such as hospital to home). With complex patients, specialists may not communicate effectively with the patient and primary or personal caregivers. These considerations underscore the need for care models in both the predischarge and postdischarge periods (as well as those linking the two periods) that increase the likelihood of safe transitions from hospital to home. (See Care models to increase safe transitions.)
COPD interventions: Exploring the evidence base
In randomized clinical trials, researchers have evaluated various care strategies to reduce readmissions in patients hospitalized for COPD exacerbations. In a systematic review of clinical trials published from January 1966 through June 2013, the author’s group identified five trials in six countries with a total of 1,393 participants (Prieto-Centurion, et al, 2014). Primary outcomes varied across the five trials and included readmission at 6 months (one trial) or 12 months (four trials); none of the trials evaluated 30-day readmissions as the primary outcome.
Each trial examined nine to eleven interventions used together as a treatment bundle in both the predischarge and postdischarge periods. The treatment bundles varied greatly across the trials. All five trials included patient education involving use of respiratory inhalers (teaching inhaler technique), development of an action plan (what to do if symptoms worsen), and provision of a hotline (contact phone number for patients to call after discharge). Other interventions that were part of some (but not all) intervention bundles included discharge planning, patient education about COPD, health counseling, providing medications for the action plan, smoking-cessation counseling, comor bidity assessment, referrals to pulmonary rehabilitation and social services, an exercise program, communication with the patient’s primary care provider, a transition navigator, home visits, and a follow-up telephone call after discharge.
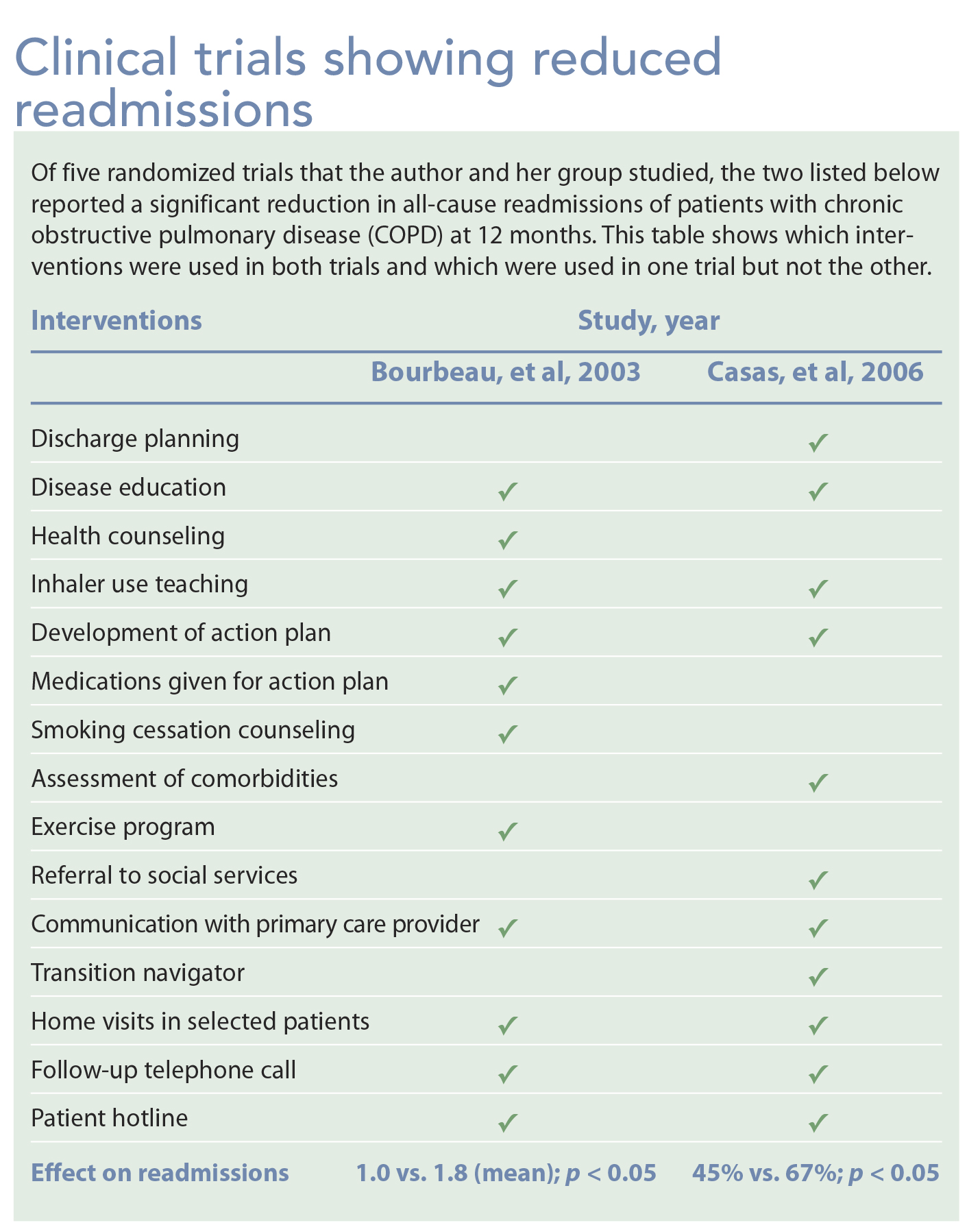
Of the five trials, two reported a significant drop in all-cause readmissions at 12 months. In addition to the three interventions used in all five trials described above, both of these trials also included disease education, communication with the patient’s primary care provider, home visits, a follow-up telephone call, and a patient hotline. (See Clinical trials showing reduced readmissions.)
Some of the following interventions were used in either the study by Bourbeau, et al or Casas, et al, but not both: discharge planning, health counseling, medications for use with the action plan, smokingcessation counseling, comorbidity assessment, exercise program, referral to social services, and use of a transition navigator to help the patient solve problems in the hospital and at home.
Other trials using bundles similar to those used by Casas and Bourbeau failed to find a reduction in readmissions (Kwok, et al, 2005; Bucknall, et al, 2012). The only trial conducted in the United States was discontinued prematurely due to an increased risk of death in the intervention group (17% vs. 7%; Fan, et al, 2012). Taken together, these findings present conflicting information on which sets of bundle interventions are effective or harmful. Possibly, some interventions are effective in some patients but harmful in others, depending on other patient-related factors (such as limited socioeconomic resources) or provider-related factors (such as limited access to postacute care).
Since publication of this systematic review, one additional clinical trial in 172 patients hospitalized for COPD exacerbations evaluated the effects of a four-intervention treatment bundle on hospital readmissions or ED visits within 30 days of discharge. The treatment bundle used in that study (Jennings, et al, 2015) consisted of inhaler education, smoking-cessation counseling, screening and referral for managing selected comorbid conditions (gastroesophageal reflux, depression, anxiety), and a follow-up telephone call after hospital discharge. This study did not detect a difference in 30-day events between the intervention and usual care groups (19% vs. 23%).
Because of CMS penalties, healthcare systems have a particular interest in 30-day rehospitalization rates for patients hospitalized for COPD exacerbations. Yet the Prieto-Centurion, et al systematic review failed to find evidence supporting a specific bundle of interventions proven to decrease 30-day readmissions. Until more definitive information is available on which intervention bundle is most effective for which patient to prevent avoidable readmissions, clinicians should take a cautious approach when implementing readmission reduction programs.
To promote a continuum of care, available evidence and clinical experience suggest the need for an interprofessional care model to implement an intervention bundle for the prehospital discharge period (before discharge home), posthospital discharge period (after hospital discharge), and to bridge the two periods (before discharge and continuing into the postdischarge period). (See CONSIDER: Provisional bundle to reduce avoidable readmissions.)
Reducing the COPD burden
We lack adequate evidence on specific interventions that can decrease 30-day all-cause hospital readmissions for COPD patients. In randomized clinical trials, no specific intervention or bundle of interventions has been shown to be consistently effective in reducing readmissions. Moreover, significant heterogeneity exists in the design and outcome measures of these clinical trials, limiting our ability to compare studies.
Programs to decrease readmissions should involve efforts to promote COPD self-management, including disease-specific education and medication instruction (such as supplemental oxygen use and inhaler technique). Initiatives should engage an interdisciplinary care team and should begin in the hospital before discharge and continuing throughout the transition to home. Based on the limited evidence available, experts recommend a provisional bundle of predischarge, postdischarge, and bridging interventions. As our case study demonstrates, clinicians also need to consider interventions directed at social determinants of health when developing care strategies for patients with COPD exacerbations. To meet the needs of complex patients, a multidisciplinary team approach is especially crucial.
Not all COPD readmissions are preventable; some patients are so ill from COPD or a comorbid condition that readmission is the most appropriate care strategy. However, the prevalence and societal burden of COPD are increasing worldwide. All nurses can benefit from understanding the significance and burden of COPD for both patients and healthcare systems.
Nina Bracken is clinical and research program manager at the Breathe Chicago Center and the Population Health Sciences Program at the University of Illinois at Chicago.
Selected references
Bourbeau J, Julien M, Maltais F, et al; Chronic Obstructive Pulmonary Disease axis of the Respiratory Network Fonds de la Recherche en Santé du Québec. Reduction of hospital utilization in patients with chronic obstructive pulmonary disease: a disease-specific self-management intervention. Arch Intern Med. 2003;163(5):585-91.
Bucknall CE, Miller G, Lloyd SM, et al. Glasgow supported self-management trial (GSuST) for patients with moderate to severe COPD: randomized controlled trial. BMJ. 2012;344:e1060.
Casas A, Troosters T, Garcia-Aymerich J, et al; members of the CHRONIC Project. Integrated care prevents hospitalisations for exacerbations in COPD patients. Eur Resp J. 2006;28(1):123-30.
Centers for Disease Control and Prevention. Chronic obstructive pulmonary disease (COPD): Data and statistics. Updated December 8, 2014.
Elixhauser A, Au DH, Podulka J. Readmissions for chronic obstructive pulmonary disease, 2008. HCUP Statistical Brief #121. September 2011.
Fan VS, Gaziano JM, Lew R, et al. A comprehensive care management program to prevent chronic obstructive pulmonary disease hospitalizations: a randomized, controlled trial. Ann Intern Med. 2012;156(10):673-83.
Feemster LC, Au DH. Penalizing hospitals for chronic obstructive pulmonary disease readmissions. Am J Respir Crit Care Med. 2014;189(6):634-9.
Fleming C. Health Policy Brief: Improving Care Transitions. Health Affairs. September 21, 2012.
Ford ES, Murphy LB, Khavjou O, et al. Total and state-specific medical and absenteeism costs of COPD among adults aged ≥ 18 years in the United States for 2010 and projections through 2020. Chest. 2015;147(1):31-45.
Global Initiative for Chronic Obstructive Lung Disease. Pocket Guide to COPD Diagnosis, Management, and Prevention: A Guide for Health Care Professionals. Seattle: CreateSpace Independent Publishing Platform; 2016.
Grippi MA, Elias JA, Fishman JA, Kotloff RM, Pack AI, Senior RM. Fishman’s Pulmonary Diseases and Disorders. 5th ed. New York: McGraw Hill; 2015.
Jennings JH, Thavarajah K, Mendez MP, Eichenhorn M, Kvale P, Yessayan L. Predischarge bundle for patients with acute exacerbations of COPD to reduce readmissions and ED visits: a randomized, controlled trial. Chest. 2015;147(5):1227-34.
Joint Commission, The. Transitions of care: The need for a more effective approach to continuing patient care. June 27, 2012.
Krishnan JA, Gussin HA, Prieto-Centurion V, Sullivan JL, Zaidi F, Thomashow BM. Integrating COPD into patient-centered hospital readmissions reduction programs. Chronic Obstr Pulm Dis (Miami). 2014;2(1):70-80.
Kwok T, Lum CM, Chan HS, Ma HM, Lee D, Woo J. A randomized, controlled trial of an intensive community nurse-supported discharge program in preventing hospital readmissions of older patients with chronic lung disease. J Am Geriatr Soc. 2004;52(8):1240-6.
Mularski RA, Asch SM, Shrank WH, et al. The quality of obstructive lung disease care for adults in the United States as measured by adherence to recommended processes. Chest. 2006;130(6):1844-50.
Prieto-Centurion V, Gussin HA, Rolle AJ, Krishnan JA. Chronic obstructive pulmonary disease readmissions at minority-serving institutions. Ann Am Thorac Soc. 2013;10(6):680-4.
Prieto-Centurion V, Markos MA, Ramey NI, et al. Interventions to reduce rehospitalizations after chronic obstructive disease exacerbations: a systematic review. Ann Am Thorac Soc. 2014;11(3):417-24.
Shah T, Churpek MM, Coca Perraillon M, Konetzka RT. Understanding why patients with COPD get readmitted; a large national study to delineate the Medicare population for the readmissions penalty expansion. Chest. 2015;147(5):1219-26.
Sharif R, Parekh TM, Pierson KS, Kuo YF, Sharma G. Predictors of early readmission among patients 40 to 64 years of age hospitalized for chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2014;11(5):685-94.
Wier LM, Elixhauser A, Pfuntner A, Au DH. Overview of hospitalizations among patients with COPD, 2008. HCUP Statistical Brief #106. February 2011. Agency for Healthcare Research and Quality.
















{kind=link}
{kind=link}
1 Comment.
I had COPD for 9 years. My first symptoms were dry cough, chest tightness and shortness of breath. My first chest x-ray only showed bronchitis. Finally I went to a pulmonologist and was diagnosed with COPD.i have used all the medication yet they don’t work, last year December I was told by a formal emphysema patient to use https://totalcureherbalfou5.wixsite.com/herbal/contact herbal treatment which I really did,i was surprise the herbal products effectively get rid of my COPD totally. When you get where you cannot breathe it may be too late. Good luck to each and every one that will be trying their herbal treatment .